
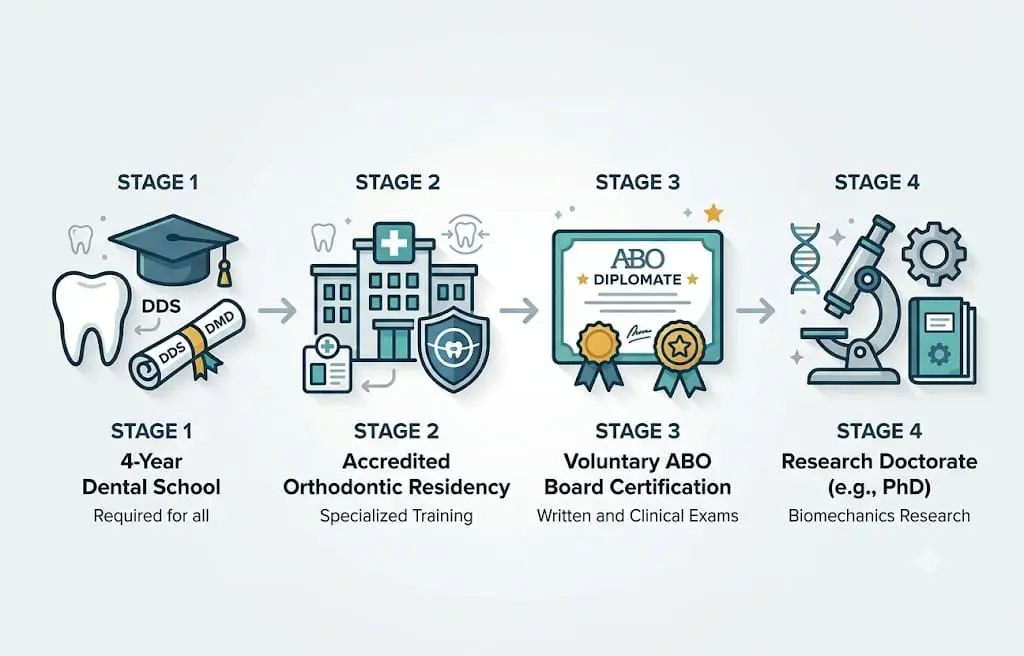
An orthodontist completes dental school plus a multi-year accredited orthodontic residency, the Specialty Certificate in Orthodontics, that a general dentist does not.
ABO Diplomate status is a voluntary board certification held by a minority of orthodontists, and a research PhD is a further academic credential. Credentials signal how much training depth stands behind the movement of teeth, matched to the complexity of the case.
Beyond clinical training, Dr. Viecilli co-invented SmartArch wire technology and has authored 27+ peer-reviewed publications. He has treated more than 5,000 cases at Limestone Hills in Austin.
That stack is not presented as the only acceptable resume. It is shown because each credential on it is verifiable, and because seeing one complete chain makes the rest of this guide concrete rather than abstract.
Every Orthodontist Is a Dentist First
The first stage of the path is identical for both providers. An orthodontist and a general dentist each complete a four-year DDS or DMD program. DDS means Doctor of Dental Surgery and DMD means Doctor of Dental Medicine. The two degrees are equivalent; only the awarding university differs.
This is why the accurate framing is Not Just a Dentist rather than the reverse. An orthodontist holds the same dental degree a general dentist holds. The distinction is what comes after dental school, not whether dental school happened.
After graduation the paths separate. A general dentist enters practice and provides routine care: exams, cleanings, fillings, crowns, root canals, and basic cosmetic work. A future orthodontist applies to a separate, competitive specialty residency focused on moving teeth and correcting bites.
The Orthodontic Residency and the Specialty Certificate
The defining credential of an orthodontist is the residency. It is a full-time, in-clinic program that runs for several years after dental school and is dedicated entirely to tooth movement, bite correction, craniofacial growth, treatment planning, biomechanics, and appliance design.
Residents treat a large volume of cases under faculty supervision before they graduate. The training is supervised, sequential, and continuous, which is the structural reason it differs from a short course taken alongside a busy general practice. A resident is in the orthodontic clinic every working day, not for a weekend.
That residency must be accredited by the Commission on Dental Accreditation (CODA), the agency recognized by the US Department of Education to accredit dental and dental-specialty education programs. A residency that meets those standards awards a Specialty Certificate in Orthodontics, the credential the American Dental Association recognizes as orthodontic specialization.
The residency is also where an orthodontist learns to plan force systems rather than only place an appliance. A resident spends years analyzing how a given tooth will respond to a given force, predicting biological response, and planning the sequence of movements. That planning skill is the part a short course cannot compress.
In Texas, only holders of that Specialty Certificate may legally call themselves orthodontists. A general dentist may still legally provide braces or aligners; the license permits the work without supplying the residency behind it. The credential, not the license, is what marks the specialty.
ABO Diplomate: The Voluntary Board Certification
The Specialty Certificate makes a clinician an orthodontist. Board certification is a separate, voluntary step on top of that. The American Board of Orthodontics (ABO) awards Diplomate status to orthodontists who pass a written examination and a clinical examination in which the doctor presents finished, documented cases to a board of examiners.
A minority of practicing orthodontists in the United States hold ABO Diplomate status. The certification is not required to practice, and many orthodontists who never pursue it are highly skilled clinicians. What it signals is a documented choice to be measured against a national peer standard rather than a guarantee of any particular outcome.
For a patient comparing orthodontists, Diplomate status is therefore a useful verifiable signal, not a verdict. It says the doctor submitted their work to external review and met the standard. It is one input among several, weighted alongside the residency, the diagnostic approach, and the plan offered for the specific case.
What a Research PhD Adds
A PhD is a research doctorate, distinct from clinical training. An orthodontist with a PhD has completed original research and contributed to the published science behind treatment, often in a field such as orthodontic biomechanics, the study of the forces that move teeth and the biological response to those forces.
This credential does not replace residency, and it does not by itself predict a clinical result. A skilled orthodontist without a PhD can produce excellent outcomes. What the research doctorate reflects is depth in the underlying mechanics rather than added chair-side hours.
Dr. Viecilli is the worked example here. His PhD is in orthodontic biomechanics, and he co-invented SmartArch wire technology, a wire system designed to deliver more efficient force across treatment. That background informs how force systems are planned, which matters most on complex movements where small mechanical choices change the outcome.
The honest framing is narrow. A research credential is evidence of depth in the science, not a marketing trophy and not a substitute for the residency that every orthodontist must complete.
Residency Versus Weekend and Continuing-Education Courses
Some general dentists complete short continuing-education courses, sometimes a weekend or a series of weekends, that introduce a clear-aligner system or basic bracket mechanics. These courses are legitimate continuing education, and a conscientious general dentist can treat straightforward cases acceptably after them.
The difference is structural, not a judgment of effort. A continuing-education course is measured in days and is taken alongside a full general practice. An accredited orthodontic residency is measured in years of full-time, supervised, in-clinic training devoted exclusively to tooth movement and bite correction.
That difference is most consequential in specific situations: complex bite problems, jaw discrepancies, impacted teeth, growing children with developing skeletal patterns, and aligner cases that need bracket support to finish precisely. In those cases, the depth of residency training is the relevant factor.
None of this makes a general dentist a poor clinician at general dentistry. The point is matching the provider’s training to the complexity of the work, not ranking the people. A great general dentist is excellent at the care general dentistry covers.
What the Credential Chain Means in the Treatment Chair
Credentials are not abstract. They translate into specific abilities a patient experiences during treatment, which is why the chain is worth understanding before choosing a provider rather than after.
Residency training shows up first in diagnosis. An orthodontist is trained to read a full set of records, including a 3D scan, and to identify whether a problem is a tooth-position issue, a jaw-relationship issue, an airway consideration, or a combination. The plan follows the diagnosis, and a wrong diagnosis produces a wrong plan no matter how the teeth are moved.
It shows up next in case selection. A large part of specialty training is recognizing which cases an aligner alone can finish, which need brackets, which need growth modification in a child, and which need surgical coordination. Knowing the limits of a tool is itself a trained skill.
It shows up last in handling the unexpected. Cases deviate from plan: a tooth resists, a root nears a neighbor, a bite shifts mid-treatment. Residency-level training is largely about predicting and managing those deviations rather than only executing a flawless plan that never meets resistance.
Board certification and a research doctorate add to that picture without changing its base. The Diplomate process forces a doctor to defend finished cases against external review, and a research doctorate deepens the understanding of why a force produces a given movement. Both reinforce the residency; neither substitutes for it.
How to Verify an Orthodontist’s Credentials
Credentials are meaningful only if they can be checked, and the strong ones are publicly verifiable. A patient does not need to take a website’s word for any of the following.
Dental licensure can be confirmed through the Texas State Board of Dental Examiners. Orthodontic residency can be confirmed by asking which program the doctor attended and checking that it is an accredited orthodontic specialty program.
ABO Diplomate status can be confirmed directly through the American Board of Orthodontics. Peer-reviewed publications and patents are searchable in public databases, so a research record is not a claim a patient has to take on faith.
A practical signal on its own is transparency. A practice that names its doctor’s dental school, residency program, board status, and research record openly makes verification simple. A page that lists the specific credential chain, the way the Limestone Hills doctor page does, is doing the disclosure work for the patient rather than asking for trust without evidence.
The Honest Limit of Credentials
Credentials are evidence of training depth. They are not a promise of a perfect result. A clinician with a long credential chain can still have a case go to refinement, and outcomes depend on diagnosis, plan, patient cooperation, and biology as much as on a resume.
A great general dentist is genuinely excellent at general dentistry, and that is not faint praise. The argument here is not status. It is fit: matching the depth of a specialist’s training to the complexity of moving teeth, and reserving that depth for the cases that actually need it.
Read that way, the credential chain is a way to set expectations honestly before treatment, not a scoreboard. The most useful question a patient can ask is whether the training behind the plan matches the difficulty of their specific case.
Austin and the Hill Country
Families across Austin and nearby communities, including Lakeway, Cedar Park, Round Rock, Bee Cave, Westlake, and Steiner Ranch, search for a board-credentialed orthodontist when treatment is on the table. The credential chain itself is universal; it does not change by city or by neighborhood.
What is local is the example. Dr. Rodrigo Viecilli at Limestone Hills is the Austin-area orthodontist whose full credential chain, ABO Diplomate, accredited orthodontic residency, PhD in orthodontic biomechanics, and a documented publication record, is laid out in plain view.
For an Austin family deciding where to start, the practical step is to read the doctor’s credentials on the Limestone Hills doctor page, then bring the specific case to a consultation where the plan, not just the resume, can be discussed.
Common Questions About Orthodontist Credentials
What credentials should an orthodontist have?
Is a board-certified orthodontist better than one who is not?
Can a general dentist do orthodontic treatment in Austin?
What does a PhD add for an orthodontist?
How can a patient verify an orthodontist’s credentials?
Sources. Commission on Dental Accreditation standards for orthodontic specialty education, American Board of Orthodontics board-certification framework, and standard dental-specialty training structure, stated qualitatively.
Specifics that could not be independently verified are stated qualitatively rather than as exact figures. Clinical observations from Limestone Hills Orthodontics, Austin, TX.
